
Hydration, Blood Flow, and the Upper Neck in POTS

Blood Volume in POTS
If you’ve ever watered a garden with a hose, you know two things matter: how much water is flowing, and whether the hose is kinked. The same is true for patients with Postural Orthostatic Tachycardia Syndrome (POTS).
Why Hydration Alone Isn’t Enough
Most of us know that drinking water is important. But here’s the key: hydration isn’t just about fluid intake — it’s about fluid retention.
If you drink water and your body immediately flushes it out, blood volume doesn’t actually increase. But when you pair water with electrolytes — especially salt — your body can hold on to that fluid. This is what allows blood vessels to carry the right amount of volume to your brain and throughout your body.
Think of it like turning up the hose so the garden actually gets watered.
How Much Salt and Water Do POTS Patients Need?
For the average person, the recommended daily sodium intake is about 2,300 mg (roughly one teaspoon of salt). That’s usually enough to keep energy steady, hydration balanced, and nerves firing properly.
But for people with POTS, the demands are higher. Because their bodies struggle to push blood to the brain and keep circulation steady, they often need 3,000 to 10,000 mg of sodium daily — along with 2–3 liters of water.
- Some may feel well with 3,000 mg.
- Others may need 5,500 mg or even 7,000+ mg.
- The exact number is individual and takes trial and error.
A good approach is to start with 3,000 mg of sodium daily and gradually increase in 500 mg steps to see where your body functions best.
The Craniocervical Connection: Flow In and Flow Out
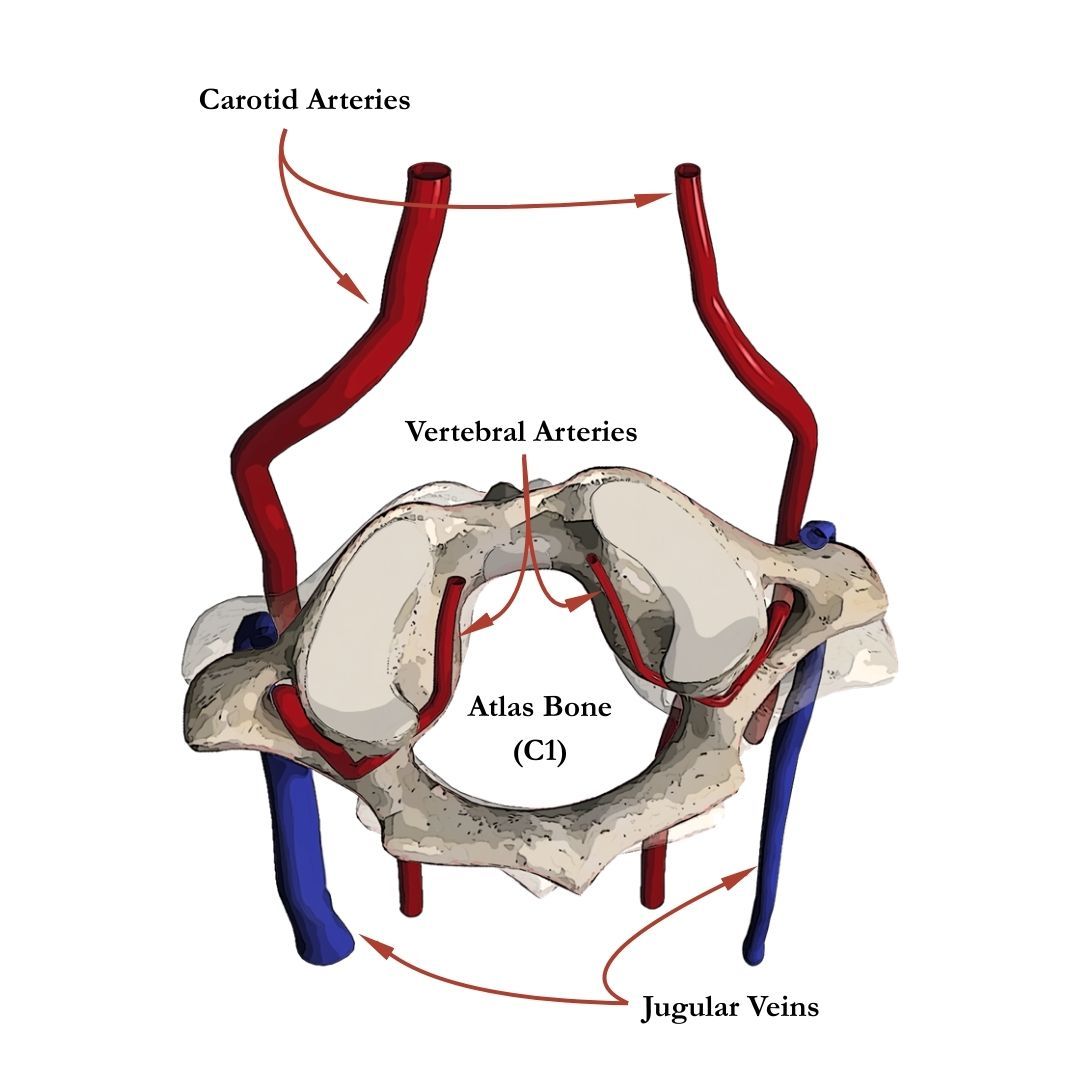
Now let’s return to the hose analogy. If you’ve got plenty of water turned on, but there’s a kink in the hose, the flow is still restricted. Notice in the image below how the right blood vessels are smaller than the left.
That’s what can happen at the craniocervical junction (CCJ) — the area where the skull meets the spine. Subtle misalignments here can affect:
- Jugular vein or vertebral artery flow.
- Cerebrospinal fluid (CSF) drainage, which is closely tied to venous outflow.
In many POTS patients, this means that while blood gets into the brain, it doesn’t drain efficiently back out. The result? Pressure in the head, migraines, dizziness, and impaired autonomic balance.
By restoring alignment at the CCJ, we often see improvements in:
- Head pressure relief
- Autonomic regulation
- Overall neurologic function
In other words, it’s not just about turning up the spigot (blood volume) — it’s also about making sure the hose is clear (unobstructed flow).
Your Recovery Starts with the Right Evaluation
Living with POTS can feel like a never-ending cycle of uncertainty and symptom management. If you’ve been searching for real answers and a more complete approach, it may be time to consider whether your upper cervical spine is part of the missing piece. At Cerebral Chiropractic Center in St. Petersburg, we specialize in identifying and correcting misalignments at the craniocervical junction that could be interfering with your autonomic function.
Call us at (727) 677-0001 or click the link below to schedule a consultation with one of our doctors. We’ll take the time to understand your history, perform a thorough evaluation, and create a precise, tailored plan to help you move toward long-term improvement.
Relevant Research
- Flanagan MF. The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurology Res Int. 2015;2015: Article ID 794829. doi: 10.1155/2015/794829. PMID: (not indexed).
- Raj SR. The postural tachycardia syndrome (POTS): pathophysiology, diagnosis & management. Indian Pacing Electrophysiol J. 2006 Apr 1;6(2):84–99. PMID: 16943900; PMCID: PMC1501099.
- Fu Q, Levine BD. Exercise and non‑pharmacological treatment of POTS. Auton Neurosci. 2018 Dec;215:20–27. doi: 10.1016/j.autneu.2018.07.001. Epub 2018 Jul 4. PMID: 30001836; PMCID: PMC6289756.
- Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology. 1993 Jan;43(1 Pt 1):132–7. doi: 10.1212/WNL.43.1_Part_1.132. PMID: 8423877.
More Articles